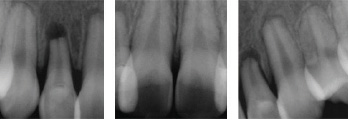
The patient was seen at our office for emergency treatment after being in a physical altercation after school. Teeth #12,11,21, and 22 were luxated and extruded in the palatal direction. No evidence of an alveolar fracture was present. The teeth were repositioned using anterior extraction forceps and digital pressure. Semi rigid splinting with a 20guage ortho wire and flowable composite was completed. The splint was removed after 3 weeks and long term follow up was advised. After 6 months, the pulps tested non-vital and root canal therapy was completed. At the 1 year follow up there was complete radiographic healing and the patient was asymptomatic and extremely grateful she could save her front teeth.